UNIQUE PHARMA QUALITY: Premium pharmaceutical grade Nandrolone Phenylpropionate (NPP) manufactured under strict GMP conditions with 99.8% purity verification.
NPP from Unique Pharma represents our commitment to delivering exceptional quality performance enhancement compounds. Each batch undergoes rigorous testing to ensure consistent potency and purity standards.
Key Characteristics of NPP
This injectable compound is administered via intramuscular injection and remains active in your system for approximately 2.5 days. Notable features include:
- Pharmaceutical grade manufacturing
- Batch-tested for purity and potency
- Consistent dosing per unit
- Optimal bioavailability
Primary Benefits:
- Enhanced performance and recovery
- Quality-assured formulation
- Reliable and consistent results
- Professional-grade compound
Mechanism of Action
Nandrolone Phenylpropionate works by interacting with androgen receptors in muscle tissue, promoting protein synthesis and nitrogen retention. This creates an optimal environment for muscle development and recovery. The compound's unique molecular structure provides specific benefits that distinguish it from other options in its class.
Usage Guidelines
Unique Pharma NPP is suitable for experienced users who understand proper cycling protocols. Always consult with a healthcare professional before beginning any supplementation regimen. Proper post-cycle therapy should be considered based on individual needs and cycle duration.
Recommended Applications
This compound is commonly incorporated into both bulking and cutting protocols depending on the user's specific goals. Its versatility makes it a popular choice among athletes and bodybuilders seeking reliable results.
Potential Considerations
As with any performance compound, users should be aware of potential effects and monitor their response accordingly. Regular health monitoring is recommended during use. Individual responses may vary based on genetics, diet, training, and other factors.
Quality Assurance
Every Unique Pharma product undergoes comprehensive quality control including:
- Raw material verification
- In-process testing
- Final product analysis
- Stability testing
Warning: Keep out of reach of children. For adults only. Not intended for use by individuals under 18 years of age.
Related products
Other Unique Pharma products
1. Description: Clinical summary
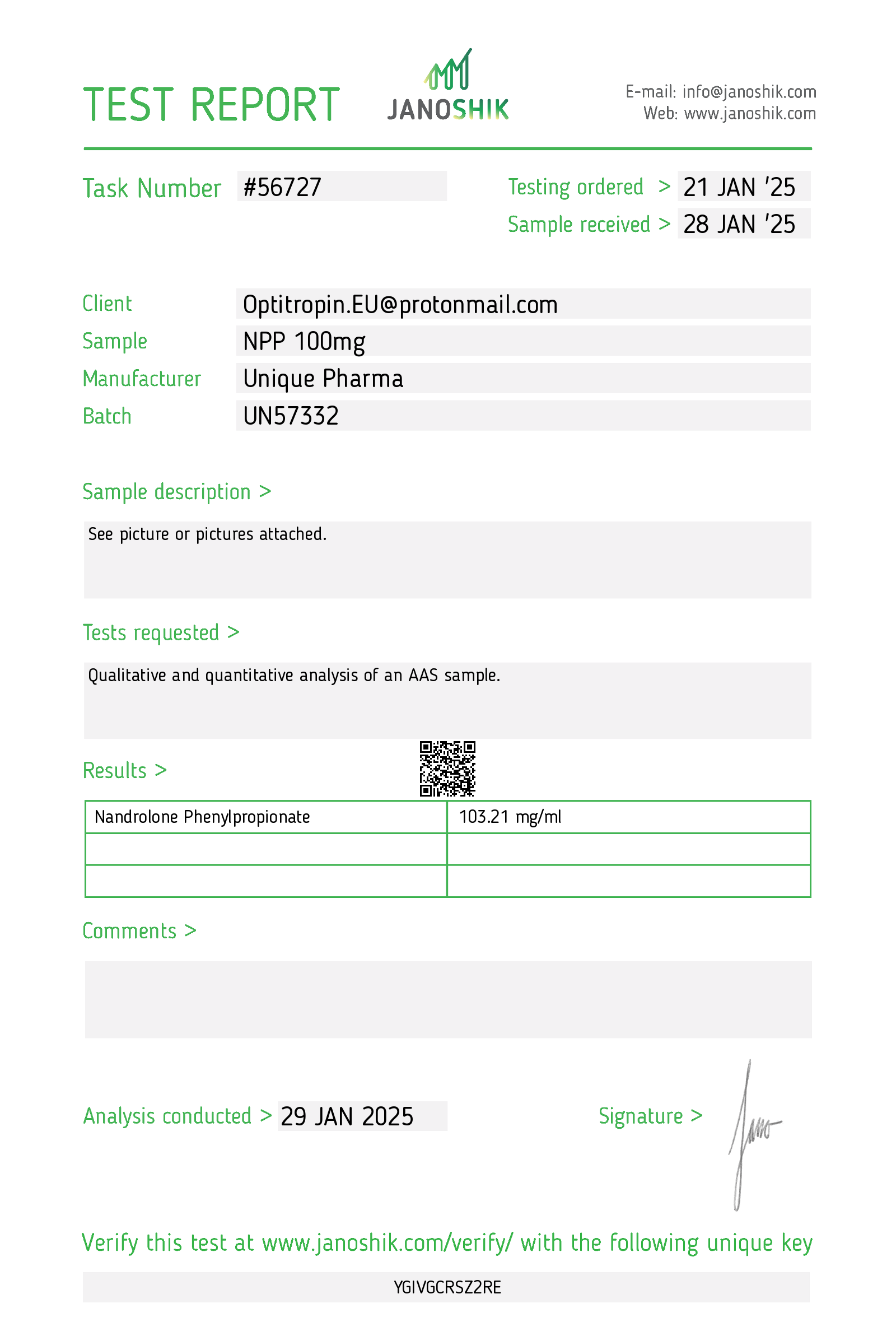
"Npp 100 mg/mL" refers to an injectable preparation containing nandrolone phenylpropionate (NPP) at a concentration of 100 mg per milliliter. Nandrolone phenylpropionate is an anabolic-androgenic steroid (AAS) — a 19‑nortestosterone derivative — esterified with the phenylpropionate moiety to prolong its activity after intramuscular administration. Historically, nandrolone esters were used in medicine for indications such as certain anemias, chronic wasting states, osteoporosis, and palliative treatment of advanced breast cancer. In modern practice, use is limited, regulated, and often replaced by other therapies. NPP is a controlled substance in many jurisdictions and should be used only under prescription and medical supervision.
Clinical formulation: oil-based injectable suspension, typical labeled strength 100 mg/mL. Intended route: intramuscular administration by or under direction of a healthcare professional.
Important legal/clinical note: Nandrolone products are controlled in many countries because of abuse potential (performance enhancement). Therapeutic use requires prescription, appropriate indications, informed consent about risks, and regular monitoring.
2. How does npp work? Mechanism of action
- Nandrolone (the active steroid after ester hydrolysis) is an agonist at androgen receptors in target tissues. Binding to intracellular androgen receptors alters gene transcription to increase protein synthesis and promote an anabolic state.
- Key pharmacodynamic effects:
- Increases nitrogen retention and net protein synthesis, supporting lean tissue maintenance and growth.
- Stimulates erythropoiesis (partly via increased erythropoietin), which can raise hemoglobin/hematocrit.
- Antagonizes some catabolic effects of glucocorticoids.
- Influences bone metabolism, which historically supported use in certain osteoporotic conditions.
- The phenylpropionate ester prolongs release from the injection site; enzymatic hydrolysis releases active nandrolone. Because the phenylpropionate ester is shorter than decanoate esters, NPP generally has a shorter apparent duration of action than nandrolone decanoate.
3. Dosage: Medical and varying usage guidelines
General principles
- Dosing must be individualized and determined by a qualified prescriber based on the indication, patient sex and age, comorbidities, and monitoring parameters.
- Before initiation: obtain baseline labs (CBC with hematocrit, liver function tests, lipid panel, PSA in men >40, pregnancy test in women of childbearing potential), cardiovascular assessment, and document contraindications.
- Route: intramuscular injection; products are for parenteral use as labeled and administered by/under clinical supervision. Do not self-administer without training and medical oversight.
Typical therapeutic dosing (historical/clinical context)
- Historically, medically supervised therapeutic doses for nandrolone esters were in the low tens to low hundreds of milligrams per dosing episode. For NPP specifically, clinical regimens used smaller, more frequent dosing than long‑acting esters because of the shorter ester. Typical therapeutic ranges reported in medical literature included on the order of tens of milligrams per dose at intervals determined by the prescribing clinician.
- Exact dose and interval must be selected by the treating physician. Do not self-prescribe or adjust dose without medical supervision.
Varying usage (off-label and performance contexts)
- Off‑label or non‑medical use (e.g., for performance or physique enhancement) often involves substantially higher doses and more frequent administration than medically indicated. Such use is associated with markedly increased risks of adverse events (cardiovascular, hepatic, psychiatric, endocrine, reproductive) and is not medically recommended.
- This guide does not provide dosing schedules for performance enhancement. If a clinician is evaluating off‑label use, risks must be discussed in detail and frequent monitoring instituted.
Monitoring during therapy
- CBC (hematocrit/hemoglobin) — baseline and periodically (risk of polycythemia).
- Liver function tests and clinical assessment for hepatic dysfunction.
- Fasting lipid panel (and management of dyslipidemia).
- Blood pressure monitoring and assessment of fluid retention.
- For men: prostate-specific antigen (PSA) and digital rectal exam as appropriate; assessment of testicular size and fertility counseling.
- For women: menstrual and virilization monitoring; pregnancy testing and teratogenic counseling.
- Psychological/behavioral assessment if mood or behavioral changes occur.
Special populations and contraindications
- Contraindicated in pregnancy (teratogenic) and breastfeeding.
- Avoid in patients with known prostate or breast cancer, uncontrolled cardiovascular disease, severe hepatic disease, and untreated severe hypertension.
- Children: use only for specific, well-justified pediatric indications under specialist supervision due to effects on growth and virilization.
4. Side effects: Common and rare adverse effects
Common and likely adverse effects
- Androgenic/virilizing effects: acne, oily skin, increased facial/body hair, voice deepening and clitoromegaly in women, menstrual irregularities.
- Endocrine suppression: decreased gonadotropin secretion leading to testicular atrophy, reduced sperm production and potential infertility in men; libido changes.
- Fluid retention and edema; weight gain related to water retention.
- Altered lipid profile: decreased HDL, increased LDL — contributing to cardiovascular risk.
- Hematologic: increased hematocrit/hemoglobin (polycythemia) — risk of thrombosis if severe.
- Injection-site reactions (localized pain, inflammation).
- Mood and psychiatric effects: mood swings, irritability, aggression, depression, emotional lability.
Less common/serious and rare effects
- Cardiovascular: hypertension, accelerated atherosclerosis, myocardial infarction, stroke — risk increased with long-term or high-dose exposure and in presence of other risk factors.
- Hepatic: clinically significant hepatotoxicity is less common with injectable 19‑nor esters than with 17‑alpha‑alkylated oral AAS, but abnormal LFTs and rare severe liver injury have been reported with anabolic steroid use.
- Gynecomastia: nandrolone has a complex aromatization/metabolite profile; gynecomastia can occur by estrogenic or progestogenic mechanisms.
- Thromboembolic events in susceptible patients.
- Allergic hypersensitivity reactions (rare).
- Long-term endocrine disruption: prolonged hypogonadism after discontinuation is possible, particularly following high-dose or prolonged use.
What to do if adverse effects occur
- Any new or severe symptoms (chest pain, severe shortness of breath, sudden vision changes, marked mood/behavior changes, jaundice, very high hematocrit, signs of thrombosis) require immediate medical evaluation.
- Mild-to-moderate side effects warrant prompt discussion with the prescribing clinician and consideration of dose adjustment, discontinuation, or supportive treatment.
5. Storage: HOW to store it
- Store at controlled room temperature unless the product label specifies otherwise — typically 20–25 °C (68–77 °F). Avoid extremes of heat and cold.
- Protect the product from light and keep the vial in its original carton until use.
- Do not freeze. If accidental freezing occurs, consult product information or the manufacturer; do not use if the formulation appears separated, cloudy (if labeled as clear), or if particulate matter is present.
- Keep out of reach of children and unauthorized persons.
- Single-use vs multi-dose vials: follow labeling. Do not use multi-dose vials beyond the period recommended on the product label. Use aseptic technique as per healthcare setting protocols; dispose of needles/syringes and unused product per local regulated medical waste rules.
- Do not store or transport with food or beverages. Dispose of expired or unused medication in accordance with local regulations — do not flush medications or discard in household trash unless allowed by local guidance.
Final clinical note
- Nandrolone phenylpropionate is a potent anabolic steroid with significant therapeutic and adverse-effect profiles. Its use must be appropriate, legal, and medically supervised. Prescribers should document indication, obtain informed consent, and perform baseline and periodic monitoring. Patients should be counseled fully on risks, contraindications (including pregnancy), potential long-term effects on fertility and cardiovascular health, and the legal status of the medication in their jurisdiction.
Note: your request names the active compound as “npp.” In clinical and pharmacologic contexts, “NPP” most commonly refers to nandrolone phenylpropionate, an esterified form of the anabolic–androgenic steroid nandrolone formulated for intramuscular injection. The guide below assumes that meaning. If you intended a different compound, tell me the exact chemical or brand name and I will revise.
1. Description: Clinical summary
Nandrolone phenylpropionate (NPP) is an androgenic–anabolic steroid (AAS) — the phenylpropionate ester of nandrolone — formulated as an intramuscular oil solution (commonly seen as 50–100 mg/mL). As an AAS, NPP produces anabolic (protein-sparing, muscle and bone-building) and androgenic (virilizing) effects. Historically it has been used in medicine for indications such as certain forms of anemia, catabolic states (cachexia), and osteoporosis, and occasionally for specific androgen-replacement uses. Because it is an androgenic steroid, NPP is a controlled substance in many jurisdictions and should only be used when prescribed by a licensed clinician for a legitimate medical indication.
Clinical characteristics
- Shorter-acting nandrolone ester compared with decanoate; designed for intramuscular injection with a relatively shorter half-life.
- Produces anabolic effects (protein synthesis, nitrogen retention, increased bone mineralization) and stimulates erythropoiesis.
- Can produce androgenic/virilizing and estrogenic-type adverse effects through aromatization and other metabolic pathways.
2. How does npp work? Mechanism of action
- Androgen receptor agonism: Nandrolone (the active moiety) binds to intracellular androgen receptors in target tissues (muscle, bone, erythroid precursors). Receptor activation modulates gene transcription that increases protein synthesis and promotes muscle growth and bone remodeling.
- Anabolic effects: Enhanced nitrogen retention, increased amino acid incorporation into protein, and stimulation of bone matrix deposition contribute to anabolic outcomes.
- Erythropoiesis: Androgens stimulate erythropoietin production and directly promote red blood cell precursor activity, increasing hemoglobin and hematocrit.
- Metabolism: Nandrolone is 5α-reduced to dihydronandrolone (DHN) in some tissues; this metabolite has lower androgen receptor activity than dihydrotestosterone (DHT), which tends to reduce some androgenic side effects relative to testosterone in some tissues. Nandrolone also aromatizes to estrogenic metabolites, though generally at lower rates than testosterone.
- Net clinical effects result from anabolic/androgenic actions and off-target metabolic effects (lipids, coagulation, endocrine feedback suppression).
3. Dosage: Medical and varying usage guidelines
Important: dosing must be individualized and prescribed by a qualified clinician. The information below is educational and is not a substitute for medical advice.
Medical (therapeutic) use
- Therapeutic regimens historically used lower, infrequent doses tailored to the indication, patient age, sex, and comorbidities. Published medical regimens for nandrolone esters have varied; when used medically the goal is to use the lowest effective dose for the shortest necessary duration.
- Example (illustrative only): Some older therapeutic protocols used nandrolone esters in the range of tens of milligrams per dose at multi‑week intervals (for example, 25–100 mg per dose given every 2–4 weeks) depending on indication. These figures are only approximate and are not a prescription.
Off‑label and non‑medical use (risk context)
- Off‑label/high-dose use (e.g., for performance or physique enhancement) often employs substantially higher and more frequent dosing than medical regimens. Such use markedly increases the risk of adverse events (endocrine suppression, cardiovascular disease, liver and psychiatric effects) and is not medically sanctioned.
- Because off‑label regimens vary widely and are associated with increased harm, they should not be undertaken outside a supervised clinical setting.
Duration and monitoring
- Duration should be determined by clinical need and tolerability. Long-term or repeated courses require regular monitoring (see Section 4).
- Prior to initiation and periodically during therapy, clinicians commonly check baseline and follow-up labs: CBC (hemoglobin/hematocrit), liver function tests, lipid profile, fasting glucose, blood pressure, and prostate-specific antigen (PSA) in men as indicated. Fertility implications should be discussed before therapy.
Legal status and prescription
- NPP (nandrolone esters) are controlled substances in many countries and are available only by prescription for approved medical indications. Use without medical supervision is illegal in many jurisdictions and dangerous to health.
4. Side effects: Common and rare adverse effects
Adverse effects can be dose-dependent. Medical supervision reduces but does not eliminate risk.
Common and expected effects
- Androgenic/virilizing: acne, oily skin, increased seborrhea, increased facial/body hair growth, androgenic alopecia (in those genetically predisposed).
- Endocrine suppression: suppression of the hypothalamic–pituitary–gonadal (HPG) axis → decreased endogenous testosterone production, testicular atrophy, impaired spermatogenesis, infertility; menstrual irregularities in females.
- Fluid-related: fluid retention, peripheral edema.
- Hematologic: increased hemoglobin/hematocrit (polycythemia) which may increase thrombotic risk.
- Injection-site reactions: pain, redness, inflammation.
- Mood/behavioral: mood swings, irritability, aggression, depressive symptoms during withdrawal.
Metabolic and cardiovascular
- Adverse changes in lipids: decreased HDL, increased LDL — adverse atherogenic profile.
- Hypertension, potential worsening of preexisting cardiovascular disease.
- Increased risk of cardiac structural changes (with prolonged/high-dose exposure).
Estrogenic effects
- Gynecomastia and breast tenderness (due to aromatization to estrogenic metabolites), though nandrolone aromatizes less than testosterone in general.
Hepatic effects
- Injectable nandrolone esters are less hepatotoxic than 17α-alkylated oral AAS, but liver function abnormalities have been reported; monitor LFTs if indicated.
Rare but serious
- Thromboembolic events (deep venous thrombosis, pulmonary embolism), particularly in the presence of polycythemia or other risk factors.
- Severe psychiatric disturbances (mania, severe aggression, suicidal ideation) in susceptible individuals.
- Exacerbation of benign prostatic hyperplasia or latent prostate cancer in men; elevation of PSA.
- Hypersensitivity reactions (rare).
Contraindications (important)
- Pregnancy and lactation (can virilize a female fetus/newborn).
- Known or suspected prostate or breast cancer.
- Uncontrolled cardiovascular disease, severe hepatic disease, or polycythemia.
- Known hypersensitivity to nandrolone or formulation excipients.
Clinical monitoring and risk mitigation
- Before and during therapy: CBC (to detect polycythemia), lipid profile, liver function tests, renal function and electrolytes as indicated, blood pressure, PSA in older men, clinical assessment for virilization, mood changes, and fluid retention.
- Counsel on fertility risks and contraception in those of reproductive potential.
- Use the lowest effective dose and shortest effective duration; discontinue or adjust if serious adverse effects occur.
5. Storage: How to store it
- Store in its original container at controlled room temperature as specified by the product labeling (typically 20–25 °C / 68–77 °F). Some formulations permit a slightly broader range; follow the manufacturer’s instructions.
- Protect from excessive heat and direct sunlight. Do not freeze.
- Keep the vial tightly closed when not in use.
- Keep out of reach of children and pets.
- Check the product’s expiration date; do not use expired medication.
- Unused or expired injectable medications should be disposed of in accordance with local regulations and healthcare facility policies (e.g., take‑back programs or hazardous pharmaceutical disposal) — do not discard sharps or injectable solutions in household trash or down drains.
Final notes and patient counseling
- Nandrolone phenylpropionate should only be used under a healthcare provider’s prescription and with appropriate baseline evaluation and ongoing monitoring.
- Discuss goals of therapy, alternatives, expected benefits, and all potential risks (particularly fertility and cardiovascular risks) before starting therapy.
- Report symptoms such as chest pain, severe headaches, sudden shortness of breath, dramatic mood changes, significant swelling, jaundice, or signs of high hematocrit to a healthcare provider immediately.
If you intended a different chemical abbreviation for “npp” (not nandrolone phenylpropionate), tell me the full name so I can prepare a tailored guide.
1. Description — Clinical summary
"NPP 100 mg/mL" is commonly used shorthand for a 100 mg/mL injectable formulation of nandrolone phenylpropionate (NPP), a synthetic anabolic–androgenic steroid (AAS). Nandrolone derivatives were developed for medical use as anabolic agents to treat conditions associated with catabolism (eg, cachexia, chronic wasting, certain anemias, osteoporosis in the past) and for some androgen-deficiency states. Most clinical uses have been superseded by other therapies in many countries, and nandrolone compounds are regulated prescription medicines in most jurisdictions.
Key points
- Formulation: intramuscular oil-based injectable, concentration often 50–100 mg/mL (here specified 100 mg/mL).
- Classification: androgen receptor agonist (anabolic steroid); has both anabolic and androgenic effects and notable progestogenic activity.
- Legal/regulatory status: prescription-only, controlled in many countries. Use should be by or under the supervision of an appropriate healthcare professional.
(If by "npp" you meant a different active compound, please confirm so I can tailor the guide.)
2. How does npp work? — Mechanism of action
- Nandrolone phenylpropionate is an esterified form of nandrolone. After intramuscular injection the ester is hydrolyzed to release the active steroid, nandrolone.
- Nandrolone binds to androgen receptors in target tissues (muscle, bone, brain, reproductive tissues), producing genomic effects (altered gene transcription) that promote protein synthesis, nitrogen retention and red blood cell production — the anabolic effects.
- Compared with testosterone:
- It has a relatively higher anabolic (tissue-building) to androgenic (masculinizing) ratio.
- It is partially aromatized to estradiol (can produce estrogenic effects such as fluid retention and gynecomastia).
- It has progestogenic activity (activation of progesterone receptors), which can augment some estrogenic side effects and suppress gonadotropin secretion.
- It is less susceptible to conversion to dihydrotestosterone (DHT) in certain tissues, which alters its androgenic profile.
- Systemic effects include erythropoiesis stimulation (increased hematocrit), alterations in lipid metabolism, and suppression of the hypothalamic–pituitary–gonadal (HPG) axis leading to reduced endogenous testosterone and sperm production.
3. Dosage — Medical and varying usage guidelines
Important: Nandrolone-containing products are prescription medications. Dosing must be individualized by a clinician, based on the indication, age, sex, comorbidities, and safety monitoring. The following are general historical/clinical reference points, not a recommendation to self-administer.
General principles
- NPP is a relatively short- to intermediate-acting ester. Shorter esters require more frequent injections to maintain steady blood levels than longer esters (eg, decanoate).
- For therapeutic uses, clinicians generally choose the lowest effective dose for the shortest necessary duration and monitor patients closely.
Examples of dosing ranges historically reported in medical literature
- Adults (therapeutic indications, historically): total doses typically in the low tens to low hundreds of milligrams per administration depending on the indication. For nandrolone esters generally reported ranges include roughly 25–100 mg per dose, with frequency determined by the ester’s half-life and the clinical context.
- Because phenylpropionate is a shorter ester than decanoate, more frequent dosing (eg, every few days) maintains steadier levels. However, many formal therapeutic regimens historically used longer esters or less frequent dosing for safety and convenience.
- Women: generally lower doses than men; careful monitoring to reduce risk of virilization.
- Children: use is generally avoided unless under specialized pediatric endocrine supervision; dosing and safety must be individualized.
Practical and safety notes
- Never self-prescribe or self-administer without physician oversight.
- Baseline assessment (see section 4) should guide dose selection and frequency.
- Duration: minimize exposure; prolonged use increases risk of HPG-axis suppression and other adverse effects.
- Discontinuation: should be supervised; abrupt cessation after prolonged use may require monitoring for hypogonadism and other effects.
If you need guidance for a specific medical indication (eg, anemia in chronic disease), provide the clinical context so the dosing information can be framed appropriately. I will not provide instructions to facilitate nonmedical or illicit use.
4. Side effects — Common and rare adverse effects
Adverse effects depend on dose, duration, sex, age, comorbidities and concomitant medications. Many effects are dose-dependent and may be reversible after stopping the drug, but some can be long-lasting.
Common/relatively frequent
- Androgenic/virilizing:
- Acne, oily skin
- Increased facial/body hair growth
- Voice deepening and clitoral enlargement (in women, potentially irreversible if prolonged)
- Fluid retention and edema
- Changes in libido and mood (irritability, aggression, mood swings)
- Injection-site reactions (pain, irritation, sterile abscess)
- Increased hematocrit/hemoglobin (polycythemia) — increased risk of thromboembolic events if severe
- Suppression of the hypothalamic–pituitary–gonadal axis:
- Reduced endogenous testosterone production in men
- Decreased sperm production and fertility (may be reversible over months)
- Lipid alterations:
- Decreased HDL cholesterol; increased LDL cholesterol — adverse cardiovascular risk profile
Less common/serious
- Gynecomastia (due to aromatization and progestogenic effects)
- Hypertension (fluid retention, changes in vascular function)
- Worsening of existing cardiac disease; increased risk of myocardial infarction and stroke over long-term/high-dose exposure (assess cardiovascular risk)
- Hepatic effects: injectable nandrolone is less hepatotoxic than many oral 17α-alkylated androgens, but liver function should still be monitored in prolonged therapy
- Psychiatric effects: severe mood disturbances, mania, depression
- Prostate effects in men: acceleration of prostate hypertrophy or cancer growth — contraindicated in known prostate cancer and requires caution in older men (monitor PSA)
- Allergic reactions (rare)
Contraindications / cautions
- Pregnancy and breastfeeding — teratogenic and virilizing for a female fetus
- Known or suspected breast cancer in men or women, prostate cancer in men
- Severe cardiovascular, hepatic or renal disease (use with caution or avoid)
- Pre-existing hypercalcemia, polycythemia, uncontrolled hypertension
- Children and adolescents — closure of epiphyses and impaired growth with use
Monitoring recommendations (typical clinical practice)
- Baseline and periodic:
- Complete blood count (monitor hematocrit/hemoglobin)
- Lipid panel (HDL, LDL, triglycerides)
- Liver function tests (ALT, AST, bilirubin as indicated)
- Serum testosterone, LH/FSH if endocrine monitoring required
- PSA in men (baseline and periodic, especially if age >40)
- Blood pressure and cardiovascular risk assessment
- Pregnancy test in women of child-bearing potential before initiation
- Monitor injection sites and watch for signs of thromboembolism, psychiatric changes, and virilization in women.
5. Storage — How to store it
- Store at controlled room temperature (typically 20–25 °C / 68–77 °F) unless manufacturer’s label specifies otherwise.
- Protect from light; keep the vial in its original carton.
- Do not freeze. Freezing may alter the oil-based formulation and syringe performance.
- Keep out of reach of children and pets.
- Use strict aseptic technique when withdrawing from vials; do not pool doses, and follow local guidance on single-use vs. multi-dose vial handling.
- Check the expiration date and do not use after expiry.
- Dispose of needles, syringes and empty vials in appropriate sharps/medical waste containers per local regulations.
Additional safety and legal notes
- Nandrolone products are controlled substances in many jurisdictions and are available only by prescription for legitimate medical indications. Misuse (non-medical use, high doses, sharing vials/needles) carries significant health risks.
- If you are taking or considering treatment with an androgen/anabolic steroid, do so only under a physician’s care with appropriate baseline assessment and ongoing monitoring.
- If you experience severe side effects (eg, chest pain, shortness of breath, severe mood changes, signs of thrombosis, jaundice, markedly elevated blood pressure), seek immediate medical attention.
If you want, I can:
- Provide a concise checklist for baseline tests and monitoring tailored to a hypothetical patient profile (eg, adult male vs. female),
- Clarify typical pharmacokinetics (half-life and expected duration of effect) for NPP,
- Or adjust this guide if by "npp" you meant a different compound.
1. Description — Clinical summary
"NPP 100 mg/mL" denotes a formulation containing nandrolone phenylpropionate (NPP) at a concentration of 100 milligrams per milliliter, typically supplied as an injectable oil-based solution. Nandrolone is an androgenic–anabolic steroid (AAS) derived from testosterone. Historically nandrolone esters have been used in prescription medicine for a limited set of indications (e.g., certain wasting states, selected anemias, and osteoporosis in some jurisdictions), but nandrolone usage and legal status vary by country. NPP is an esterified nandrolone with a relatively short ester compared with decanoate, giving a shorter duration of action than longer esters.
NPP is a prescription-only medication in most places. Use should be supervised by a qualified clinician, with pretreatment assessment and ongoing monitoring for efficacy and adverse effects.
2. How does npp work? — Mechanism of action
- Nandrolone is an agonist at the androgen receptor (AR). Activation of AR in target tissues increases transcription of genes that promote protein synthesis and nitrogen retention, producing anabolic effects on muscle and bone.
- Compared with testosterone, nandrolone has relatively strong anabolic effects and reduced androgenic effects in some tissues. It also exhibits progestogenic activity through interaction with progesterone receptors, which can contribute to suppression of the hypothalamic–pituitary–gonadal (HPG) axis.
- Metabolism: nandrolone is partially reduced by 5α‑reductase to dihydronandrolone (DHN), a less androgenic metabolite; it is also aromatized to estrogens to a lesser extent than testosterone. These metabolic pathways influence both therapeutic actions and adverse-effect profiles (e.g., estrogenic effects, suppression of gonadotropins).
- Systemic effects include anabolic effects (bone density, lean body mass) and endocrine effects (negative feedback on luteinizing hormone [LH] and follicle-stimulating hormone [FSH], which may reduce endogenous testosterone production and spermatogenesis).
3. Dosage — Medical and varying usage guidelines
Important principles:
- NPP is prescription-only. Dosing must be individualized by a clinician based on the indication, patient age, sex, comorbidities, laboratory values, and response.
- The concentration "100 mg/mL" means each milliliter of solution contains 100 mg of active nandrolone phenylpropionate. Dose is therefore expressed in mg (not mL).
Medical/therapeutic use:
- Therapeutic regimens historically used for approved indications have employed comparatively low and intermittent dosing under close supervision. Treatment frequency and dose are determined to achieve clinical benefit while minimizing adverse effects and are tailored to the indication.
- Clinicians will routinely reassess risk/benefit, monitor laboratory tests (hematocrit/hemoglobin, liver function, lipids, PSA in men, endocrine function), and adjust or discontinue therapy if safety signals emerge.
Off‑label and non‑medical use:
- Use of nandrolone for performance enhancement, cosmetic muscle-building, or other non‑approved purposes frequently involves higher doses and more frequent administration than therapeutic regimens and carries substantially increased risks (cardiovascular, endocrine, psychiatric, hepatic, and reproductive). Such use is not medically recommended and is often illegal depending on jurisdiction.
- If a patient is considering or has used nandrolone for non‑medical purposes, they should be encouraged to disclose this to their healthcare provider so appropriate monitoring and harm-reduction measures can be implemented.
Monitoring and duration:
- Prior to starting therapy: baseline CBC, liver function tests, fasting lipids, blood pressure, renal function as indicated, pregnancy test in people of childbearing potential, and relevant tumor markers (e.g., PSA) if indicated.
- During therapy: periodic monitoring of hematocrit/hemoglobin (risk of erythrocytosis), lipids (possible HDL decrease/LDL increase), liver enzymes, blood pressure, and endocrine parameters. Frequency is individualized but often includes checks within weeks of initiation and periodically thereafter.
- Treatment duration depends on indication and response; long-term therapy increases cumulative risk.
Administration route:
- NPP is formulated for intramuscular injection. Administration should be performed by trained healthcare personnel or by a patient trained and authorized to self-administer by their clinician; proper sterile technique and safe sharps disposal are required.
Because dosing must be individualized and is prescription-restricted, this guide does not provide specific numeric regimens for unsupervised use. Consult a licensed clinician for a regimen tailored to the patient’s condition and monitoring plan.
4. Side effects — Common and rare adverse effects
Common/relatively frequent adverse effects
- Endocrine/reproductive:
- Suppression of the HPG axis → decreased endogenous testosterone, testicular atrophy, reduced sperm production/fertility.
- Menstrual irregularities or amenorrhea and virilization in women (voice deepening, clitoromegaly, hirsutism).
- Dermatologic:
- Acne, increased oiliness of skin, oily hair; injection‑site reactions (pain, swelling).
- Fluid/electrolyte:
- Fluid retention and edema; may exacerbate congestive heart failure or hypertension.
- Hematologic:
- Increased hematocrit/hemoglobin (erythrocytosis) with thrombotic risk if untreated.
- Cardiometabolic:
- Adverse lipid profile changes (decreased HDL, increased LDL), potential rise in blood pressure.
- Psychological/behavioral:
- Mood changes, irritability, aggressive behavior, mood instability.
Less common/serious but important adverse effects
- Cardiovascular events: ischemic heart disease, stroke, cardiomyopathy; risk increases with prolonged/high‑dose use and with preexisting risk factors.
- Prostate effects: enlargement and possible stimulation of occult prostate cancer in men; monitor PSA.
- Hepatic effects: injectable nandrolone is less hepatotoxic than 17‑alpha‑alkylated oral AAS, but idiosyncratic liver injury and cholestasis have been reported with anabolic steroids; monitor LFTs if clinically indicated.
- Thromboembolic events: deep vein thrombosis, pulmonary embolism — rare but serious.
- Allergic/hypersensitivity reactions: rare immediate hypersensitivity to excipients or the active agent.
- Long-term endocrine effects: persistent hypogonadism following prolonged use, with protracted recovery of fertility in some cases.
Contraindications and precautions
- Contraindicated in pregnancy and lactation (risk of fetal virilization).
- Contraindicated in patients with known androgen-sensitive cancers (e.g., prostate or male breast cancer) or suspected hormone-dependent tumors.
- Use with caution in patients with severe cardiac, renal, or hepatic disease, uncontrolled hypertension, polycythemia, or a history of thromboembolic disease.
- Drug interactions: may interact with anticoagulants (altered warfarin effect), insulin and oral antidiabetic drugs (glucose/insulin sensitivity changes), corticosteroids, and other androgenic agents. Always review concomitant medications.
If adverse effects occur, discontinue and consult a clinician immediately. Emergency care is indicated for signs of thrombosis, severe jaundice, acute cardiac symptoms, or severe allergic reaction.
5. Storage — How to store it
- Store at controlled room temperature as specified by the manufacturer (commonly 15–30 °C / 59–86 °F). Do not freeze.
- Protect from excessive heat and light; keep in original container until use.
- Keep out of reach of children and pets.
- Do not use injectable product if the solution is discolored, cloudy, or contains particulate matter, or if the container is damaged, prior to consulting a pharmacist or clinician.
- Dispose of unused medicine and sharps (needles, syringes) safely according to local regulations or take-back programs. Never dispose of needles in household trash without appropriate sharps containers.
Final notes
- This guide is educational and does not replace individualized medical advice. Nandrolone phenylpropionate is a prescription-controlled medication in many jurisdictions. Discuss indications, contraindications, monitoring, and legal status with a licensed healthcare provider before any use.
1. Description — Clinical summary
"Npp 100 mg / mL" (active compound: npp) commonly refers to nandrolone phenylpropionate (NPP), a short‑acting ester of the anabolic androgenic steroid nandrolone formulated for intramuscular injection. Nandrolone is an androgen with pronounced anabolic (tissue‑building) effects and relatively lower androgenic activity than testosterone.
Medically, nandrolone esters have been used for a variety of indications historically, including certain anemias, catabolic states (severe weight loss, cachexia), chronic debilitating disease, and osteoporosis. Many countries restrict nandrolone to prescription use because of potential harms and its anabolic steroid classification. NPP is shorter‑acting than nandrolone decanoate; it is typically provided as an oil‑based injectable solution.
Important: NPP is a prescription medication. Its use should be under the supervision of a qualified clinician; non‑medical use (performance enhancement) is associated with legal and health risks.
2. How does npp work? — Mechanism of action
- Nandrolone (the active steroid) binds to androgen receptors in target tissues (muscle, bone, bone marrow, etc.), initiating gene transcription that increases protein synthesis and nitrogen retention—this underlies anabolic effects such as increased lean body mass and improved bone mineralization.
- It stimulates erythropoiesis (red blood cell production), partly via effects on the bone marrow and possibly via increased erythropoietin, which can raise hemoglobin/hematocrit.
- Nandrolone can be aromatized to estrogenic metabolites (but to a lesser extent than testosterone), and it also has progestogenic activity via the progesterone receptor. Both estrogenic and progestogenic activities contribute to certain adverse effects (e.g., gynecomastia risk).
- Nandrolone exerts negative feedback on the hypothalamic–pituitary–gonadal (HPG) axis, suppressing luteinizing hormone (LH) and follicle‑stimulating hormone (FSH), which can reduce endogenous testosterone production and impair spermatogenesis.
3. Dosage — Medical and varying usage guidelines
General principles
- Dosage must be individualized based on the treated condition, patient age, sex, comorbidities, and laboratory monitoring. Only use under a prescriber’s guidance.
- Route: intramuscular injection (oil solution). Frequency varies with clinical need and ester half‑life.
- The following are approximate therapeutic ranges reported historically for nandrolone esters; they are presented for clinical context only and do not replace a prescription.
Typical therapeutic dosing (examples from clinical literature/practice)
- Low-to-moderate therapy (e.g., certain anemias, catabolic states): approximately 25–50 mg per injection at intervals such as every 2–4 weeks.
- More active replacement or severe catabolic states: some regimens have used up to 50–100 mg per injection with dosing intervals individualized (e.g., every 1–2 weeks). Higher or more frequent dosing increases adverse effects and requires close monitoring.
Important safety and monitoring recommendations
- Start with the lowest effective dose and reassess clinical benefit and adverse effects frequently.
- Baseline and periodic monitoring are recommended: complete blood count (CBC) including hematocrit, liver function tests, fasting lipid profile (HDL/LDL), blood pressure, PSA in men (if age appropriate), and assessment of mood/behavioral changes. For long‑term use, monitor bone mineral density and reproductive function as indicated.
- Contraindications include androgen‑sensitive prostate or breast cancer, pregnancy or potential pregnancy (risk of virilization of female fetus), untreated severe cardiac, hepatic, or renal disease, and uncontrolled polycythemia.
- Inform patients about effects on fertility (possible reversible or sometimes prolonged suppression of spermatogenesis) and potential virilization in women (hirsutism, voice deepening, clitoral enlargement), which may be irreversible.
- Avoid concurrent unmonitored use with other androgens or anabolic agents.
Legal and clinical note
- Dosing used for athletic or bodybuilding performance is typically substantially higher than therapeutic doses and is associated with greater health risks; such non‑prescribed use is illegal in many jurisdictions and outside established medical practice.
- Any dosing regimen should be prescribed and supervised by a licensed clinician with appropriate monitoring.
4. Side effects — Common and rare adverse effects
Common/expected adverse effects
- Androgenic/virilizing: acne, oily skin, increased facial/body hair, male‑pattern hair loss (in genetically susceptible males), voice deepening and menstrual irregularities or hirsutism in women.
- Endocrine/reproductive: suppression of endogenous testosterone production, testicular atrophy, reduced sperm production and fertility.
- Fluid retention and edema (can exacerbate hypertension or heart failure).
- Increased red blood cell mass (erythrocytosis/polycythemia) — raises thrombotic risk if unmonitored.
- Mood and neuropsychiatric effects: irritability, mood swings, aggression, depression in some patients.
- Metabolic: unfavorable changes in lipid profile (↓ HDL, ↑ LDL), possible increases in blood pressure.
Less common/serious and rare adverse effects
- Hepatic effects: injectable nandrolone is less hepatotoxic than some oral 17‑alkylated androgens, but liver function should still be monitored. Rarely cholestasis or hepatic dysfunction may occur.
- Cardiovascular events: increased cardiovascular risk (myocardial infarction, stroke) especially with long‑term or high‑dose use due to lipid and hemodynamic effects.
- Thromboembolic events secondary to polycythemia.
- Allergic reactions at the injection site or systemic hypersensitivity (rare).
- Potential stimulation of androgen‑sensitive malignancies (contraindicated in known prostate or breast cancer).
Drug interactions and special populations
- Use caution with anticoagulants (androgens may alter coagulation), insulin or oral hypoglycemics (androgens can change glucose tolerance), and corticosteroids (additive anabolic/catabolic interactions).
- Pregnancy: contraindicated due to virilization risk to female fetuses.
- Children/adolescents: can cause premature epiphyseal closure and stunted linear growth — generally contraindicated except in specific, supervised pediatric indications.
When to seek urgent care
- Signs of jaundice, severe abdominal pain, sudden severe headache or focal neurological signs, chest pain, shortness of breath, sudden leg swelling/pain (possible thrombosis), severe depression or suicidal ideation, or any signs of severe allergic reaction.
5. Storage — How to store it
- Store the drug in its original container at controlled room temperature (commonly 20–25 °C / 68–77 °F) unless the product label specifies otherwise. Short excursions outside this range are often acceptable per manufacturer guidance.
- Protect from light and excessive heat. Do not freeze oil‑based injectable formulations.
- Keep the vial sealed and sterile until use. Do not use if product appears discolored, cloudy (if it should be clear), or contains particulate matter not specified by the manufacturer.
- Keep out of reach of children and pets.
- Follow local regulations for disposal of unused medication and for sharps disposal (used needles/syringes must be disposed of in approved sharps containers per local rules).
Final important points
- NPP (nandrolone phenylpropionate) is a prescription medication with potential for significant adverse effects and legal controls. Use only when prescribed by a qualified clinician, follow monitoring recommendations, and report any adverse effects promptly. Do not use for performance enhancement or without medical oversight.